

Surgical Dermatology- Mohs Micrographic Surgery
Dr. Murakawa specializes in Mohs micrographic surgery and has an extensive background in this highly successful procedure. Mohs micrographic surgery offers the highest cure rates for basal cell carcinoma and other skin cancers, with a cure rate of 97-99% for all malignancies.
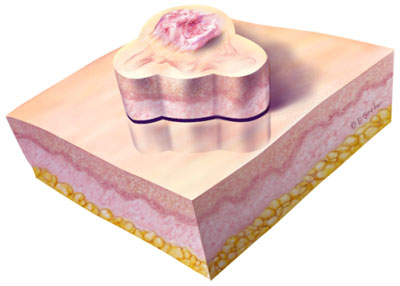
Mohs is a tissue-sparing procedure that limits the size of the surgical defect. Also, since large tumors often require flaps and grafts for repair, reassurance that the tumor is completely excised prior to repair is optimal.
Most tumors on the face, ears, head, and neck can be excised by Mohs. Appropriate indications include tumors on the central face (around the eyes, nose, mouth) and ears; large tumors (>2 cm); recurrent or incompletely excised tumors; aggressive tumors (micronodular, infiltrative, morpheaform, and basosquamous tumors); and tumors with perineural invasion. We are happy to work with plastic surgeons for surgical defects. However, we surgically repair most of our defects, and routinely perform flaps and grafts on large defects.
Mohs F.A.Q.What are Basal Cell and Squamous Cell Carcinoma? How do I prepare for the day of surgery? What happens the day of surgery? What can I expect after the surgery is complete? Will I develop more skin cancers?
Cancer is the abnormal growth of cells at an uncontrolled and unpredictable rate. The cancer tissue usually grows at the expense of surrounding normal tissue. In the skin, the most common types of cancer are basal cell and squamous cell . The names reflect the cell within the skin from which the particular type of skin cancer originates. In the Mohs Surgery Clinics we treat basal cell carcinomas, squamous cell carcinomas, and some much rarer skin tumors. Malignant Melanoma or a "cancerous mole" is a rarer type of skin cancer that usually appears as a dark colored spot or bump on your skin and which slowly enlarges. What are Basal Cell and Squamous Cell ? Both of these cancers behave and are treated in a similar manner. Their difference lies in the cell from which they originate within the skin. Often, this can only be distinguished by examining the skin under a microscope. Basal cell carcinoma is the most common cancer of any type. Both basal cell carcinoma and squamous cell carcinoma come from the words "chemical" and "surgery". The addition of "Mohs" honors the doctor who developed the technique. It is a highly specialized form of treatment for the total removal of skin cancers. It is performed by a team of medical personnel, which includes physicians, nurses, and a technician. The physician heading the team has had surgical training in the technique. The nurse is an important part of the team who will help answer your questions, responds to your anxieties, assists in surgery, and instructs you in dressings and would care after the surgery is performed. A technician, whom you may not even meet, performs the essential task of preparing the tissue slides that are examined under a microscope by the physician. The word "chemosurgery" as used today is really a misnomer. When Dr. Mohs initially introduced the procedure, he applied a chemical (zinc chloride) to the tumor and surrounding skin, which fixed the tissue prior to its removal. In the last 10 years, the procedure has been refined and improved upon so that most cases are done using fresh tissue (omitting the chemical paste). The name given to the original technique is Mohs Chemosurgery: fixed tissue technique. The majority of cases today are done using Mohs Chemosurgery: fresh tissue modification. We prefer to drop the "chemo", calling the technique Mohs Surgery. The surgery is performed as follows: the skin suspicious for cancer is treated with a local anesthetic so there is no feeling of pain in the area. To remove most of the visible skin cancer, the tumor is scraped using, a sharp instrument called a curette. A thin piece of tissue is then removed surgically around the scraped skin and carefully divided into pieces that will fit on a microscope slide; the edges are marked with colored dyes; a careful map or diagram of the tissue removed is made; and the tissue is frozen by the technician. Thin slices can then be made from the frozen tissue and examined by the doctor under the microscope. Most bleeding is controlled using pressure and other routine measures, although occasionally a small blood vessel is encountered which must be tied using suture material. A pressure dressing is then applied and the patient is asked to wait while the slides are being, processed. The physician will then examine the slides under the microscope and be able to tell if any tumor is still present. If cancer cells remain, he is able to exactly locate them based upon his map. Another layer of tissue is then removed and the procedure is repeated until the physician is satisfied that the entire base and sides of the wound have no cancer cells remaining. As well as ensuring total removal of the cancer, this process preserves as much normal, healthy, surrounding skin as possible. The removal of each layer of tissue takes approximately one to two hours. Only 20 to 30 minutes of that is spent in the actual surgical procedure, the remaining time being required for slide preparation and interpretation. It usually takes removal of two or three layers of tissue (called "stages"), to complete the surgery. Therefore, by beginning early in the morning. Mohs Surgery is generally finished in one day. Sometimes, however, a tumor may be extensive enough to necessitate continuing surgery a second day. At the end of Mohs Surgery, you will be left with a surgical wound. This wound will be dealt with in one of several ways. The several options will be discussed with you in order to provide the best possible cosmetic results without disguising the small possibility of recurrence. The possibilities explained below include: 1. Healing by spontaneous granulation; 2. Closing the wound, or part of the wound with stitches; 3. Using a skin graft; 4. Using a skin flap; or 5. Arranging a consultation with a surgeon who specializes in more complicated surgical repairs. Healing by spontaneous granulation involves letting the wound heal by itself. This offers a good chance to observe the wound as it heals after removal of a difficult tumor. Experience has taught us that there are certain areas of the body where nature will heal a wound as nicely as any further surgical procedure. There are also times when a wound will be left to heal knowing, that if the resultant scar is unacceptable, some form of cosmetic surgery can be performed at a later date. Closing the wound with stitches is often performed on a small lesion. This involves some adjustment of the wound and sewing the skin edges together. This procedure speeds healing and can offer a good cosmetic result. For example, the scar can be hidden in a wrinkle line. Skin grafts involve covering a surgery site with skin from another area of the body. There are two types of skin grafts. The first is called a split-thickness graft. This is a thin shave of skin, usually taken from the thigh, which is used to cover a surgical wound. This can be either a permanent coverage or temporary coverage before another cosmetic procedure is done at a later date. The second graft-type is the full-thickness graft. This graft provides a thicker layer of skin to achieve proper results. In this instance, skin is usually removed from behind the ear or around the collarbone (the donor site), and stitched to cover a wound. The donor site is then sutured together to provide a good cosmetic result. Skin flaps involve movement of adjacent, healthy tissue to cover a surgical site. Where practical, they are chosen because of the excellent cosmetic match of nearby skin. If your Mohs Surgery is extensive or is performed where a functional impairment results, we may recommend you visit one of several consultant physicians. If you have been sent to us by a physician skilled in skin closures (for example, a plastic surgeon), he or she will take care of you after your cancer has been removed. In summary, by microscopically pinpointing, areas involved with cancer and selectively removing these tissues, the Mohs surgeon can successfully remove your skin cancer. Because normal tissue is preserved to the greatest extent possible, the Mohs surgeon is able to offer you the possibility of a good cosmetic result. Although an attempt will be made to minimize the scar, you will be left with a scar of some kind. How do I prepare for the day of surgery? The best preparation for Mohs Surgery is a good nights rest followed by breakfast. In most cases, the surgery will be completed on an outpatient basis. Because you can expect to be here for most of the day, it is wise to bring a book or magazine to read. Also, because the day may prove to be quite tiring, it is advisable to have someone accompany you on the day of surgery to provide companionship and to drive home. Your referring physician may request that you have a preoperative visit to evaluate the need for Mohs Surgery. At this visit, the technique will be discussed in detail, you will meet the "team" performing the surgery, and a biopsy may be performed. If you are traveling a great distance and/or are being referred by a physician familiar with the technique, you may be referred directly for Mohs Surgery without a preoperative visit. If this is the case, and you have never been a patient at Somerset Skin Centre before, you should plan to arrive 20 to 30 minutes before your scheduled appointment in order to register. If you take any medications, bring them with you in their labeled bottles or tubes. We request that you stop taking any aspirin or aspirin containing compounds (like Anacin, Bufferin, or Ascriptin) at least a week before your surgery. This is because they may interfere with the normal blood clotting mechanism, making you bleed more than normal during surgery. What happens the day of surgery? Your appointment has purposely been scheduled early in the day. When the surgical suite becomes available, our nurse will escort you to that area of the clinic. After preliminary preparation of the skin, you will be placed on the surgical table and the area around your skin cancer will be anesthetized (numbed) using a local anesthetic. This may be uncomfortable, but usually this is the only pain you will feel during the procedure. Once the area is numbed, a layer of tissue will be removed and the bleeding controlled. The layer of tissue removed will be carefully handled by the surgeon, diagrammed, and sent to the technician to be processed into microscopic slides. A pressure dressing will be placed over your surgical wound and you will be free to leave the surgical suite. On the average, it takes an hour for the slides to be prepared and studied. During this time you may wait in the waiting room, read your book or magazine, or take a walk around the medical center. Most Mohs Surgery cases are completed in two or three stages. Each stage involves the removal and microscopic examination of your skin for cancer. Therefore, the majority of cases are finished during one day. Once we are sure that we have totally removed your skin cancer, we will discuss with you our recommendations for dealing with your surgical wound. What can I expect after the surgery is complete? Most people are concerned about pain. You will experience remarkably little discomfort after your surgery. Due to its potential to cause bleeding, we request that you do not take aspirin, but use Tylenol or a Tylenol-like painkiller (Datril). Rarely, a stronger pain medicine will be prescribed. Bleeding A small number of patients will experience some bleeding post operatively. This bleeding can usually be controlled by the use of pressure. You should take a gauze pad and apply constant pressure over the bleeding, point for 15 minutes; do not lift up or relieve the pressure at all during that period of time. If bleeding persists after continued pressure for 15 minutes, repeat the pressure for another 15 minutes. If this fails, call your physician or visit a local urgent care facility. Complications There are some minor complications which may occur after Mohs Surgery. A small red area may develop surrounding your wound. This is normal and does not necessarily indicate infection. However, if this redness does not subside in two days or the wound begins to drain pus, you should notify your physician immediately. Itching and redness around the wound, especially in areas where adhesive tape has been applied, are not uncommon. When this occurs, ask your druggist for a non-allergenic tape and tell us on your return visit, Swelling and Bruising are very common following Mohs Surgery, particularly when it is performed around the eyes. This usually subsides within four to five days after surgery and may be decreased by the use of an ice pack in the first 24 hours. At times, the area surrounding your operative site will be numb to the touch. This area of anesthesia (numbness) may persist for several months or longer. In some instances, it may be permanent. If this occurs, please discuss it with your physician at your follow-up visit. Although every effort will be made to offer the best possible cosmetic result, you will be left with a scar. The scar can be minimized by the proper Wound Care Information Sheets which will explicitly outline how to take care of whatever type of wound you have. Most Mohs Surgery cases are completed in two or three stages. Each stage involves the removal and microscopic examination of your skin for cancer. Therefore, the majority of cases are finished during one day. Once we are sure that we have totally removed your skin cancer, we will discuss with you our recommendations for dealing with your surgical wound. Will I develop more skin cancers? After having one skin cancer, statistics say that you
have a higher chance of developing a second. The damage
which your skin has already received from the sun cannot
be reversed. However, there are precautions that can
be taken to prevent further skin cancers. They involve
good common sense. You should use a sunscreen (suntan
lotion) applying it at least 10 minutes before exposure
to sunlight. The sunscreens are now labeled as to strength;
the higher numbers are more protective. We would recommend
that you use #15 or higher sunscreen. Despite manufacturer's
claims, we recommend that you reapply sunscreen after
swimming. A wide brimmed hat, long-sleeved shirt and
other protective clothing are also appropriate. Avoidance
of excessive sunshine is recommended. You should have
your skin checked very closely by a physician at six-month
intervals. This is not only to check the surgical site
as it is healing, but also to check for the development
of additional skin cancers. Our policy is for us to
follow the majority of our patients until the wound
has healed, and then they can continue to be followed
very well by their referring physician. We recommend
six-month follow-up visits for two years, then yearly.
Of course, any areas of your skin that change, fail
to heal, or just concern you should be brought to the
attention of your referring physician immediately. He/She
will be able to adequately treat most skin cancers when
they are detected early and are small. Billing for Somerset Skin Centre is based on a standard fee schedule dictated by Medicare and the insurance companies. Coverage will depend on your insurance plan. Should you have any questions regarding coverage, please contact your insurance company for assistance. If you are being referred under a prepaid insurance program, such as a health maintenance organization (HMO), we are not permitted to treat any condition that has not been specifically requested by your primary care physician. Please make sure to have the referral information taken care of before your appointment to prevent any unnecessary delays. If you have any questions regarding the billing, please call our office at (248) 244-8448. |